
Alice Roberts
The Incredible Unlikeliness of Being: Evolution and the Making of Us
Heron Books, 2014
 Alice Roberts is Professor of Public Engagement with Science at the University of Birmingham, and is perhaps the outstanding scientific polymath of our age: medic, anatomist, anthropologist, archaeologist, television science presenter and no mean artist. The Incredible Unlikeliness of Being is her latest book and sets out to unfold for us the amazing way in which we develop as an embryo and foetus and some of the ways in which we have probably evolved to this. And what an amazing voyage we are taken on!
Alice Roberts is Professor of Public Engagement with Science at the University of Birmingham, and is perhaps the outstanding scientific polymath of our age: medic, anatomist, anthropologist, archaeologist, television science presenter and no mean artist. The Incredible Unlikeliness of Being is her latest book and sets out to unfold for us the amazing way in which we develop as an embryo and foetus and some of the ways in which we have probably evolved to this. And what an amazing voyage we are taken on!
I found the book immensely interesting and very readable. Roberts’ style is light, airy and chattily personal, while being scientifically accurate and informative — at times amusing and even ribald: how many authors could get away with a section entitled “Mind the Bollocks”? In fact I found the book so readable I had to ration myself to one or two chapters a night otherwise I would have devoured it in a single all night read.
We are taken on a journey from conception to birth with a look at how all the major systems of the body develop throughout pregnancy from the single egg and the successful sperm to the birth of a baby. Along the way Roberts describes the embryology, including insights from her own two pregnancies and the medical tests she has had done on her in the interests of science.
But more than this, she also discusses the archaeological evidence for how and why evolution has given us the kit of parts we have; how evolution got to produce them; and why they are different from other species. Right at the beginning of the book Roberts discusses the various theories of embryos and how babies are built from Aristotle to the present day. She is at pains to point out that each of these theories was consistent with the state of knowledge at the time so we shouldn’t scoff at them for being ignorant — one day our theories will be considered equally backward in the light of new knowledge.
Yes, I thoroughly enjoyed this book, but that doesn’t mean I don’t have reservations about it. It is a book for the scientifically (specifically, medically) literate layman. Roberts, rightly in my view, calls things by their correct scientific and medical names but I felt too often missed the opportunity to explain those names; what the part is or does. Of course the downside of providing more explanation is that it could disrupt the flow of the text (and make for a larger, more expensive book).
However I think there is a solution, at least in part, to this problem. The book is illustrated by Roberts’ own delightful line drawings — a very real demonstration of her skill as an anatomist! But there are for my money far too few illustrations. There were many occasions where I felt that a drawing (or other illustration) could have made the text much more powerful: especially in cases where the anatomy of different species, or at different stages of development, is being compared. Yes, some of those drawings are there, but for me too few. And drawings could have been used to explain some of the otherwise unexplained. In this respect I wanted more.
My other gripe is one which I all too frequently have to level at modern publishing (rather than authors): the poor quality of the paper used. Yes everyone wants to keep cost down and at £19.99 for almost 400 pages in hardback this is at the cheaper end of the spectrum. But oh that poor quality paper, which will not stand the test of time.
These are, however, relatively minor complaints about a book which I found informative, hugely interesting and immensely readable. I definitely came out somewhere different to where I went in!
So if you are interested in how babies grow in the womb, and how we got to be the shape we are, then I would thoroughly recommend this book.
It really is just so unlikely that we are all here, and as “normal” as we are!
Overall Rating: ★★★★★
Category Archives: medical
Welsh Cannabis
Following on from the previous post about the liberalisation of prostitution, here’s another piece of unexpected sensible news.
The NHS in Wales will be the first in the UK to fund a cannabis-based medicine for people with multiple sclerosis. The drug in question is Sativex which has been on the market for some time.
Bravo for them as this is in line with current medical research, but directly contrary to the the recent draft NICE clinical guideline which rejected the drug for use on the NHS in Wales and England based, apparently, on a flawed assessment of its cost effectiveness.
You see, by chipping away, entrenched attitudes can be changed.
Wales 1, Blinkered Politicians 0
Your Interesting Links
Another selection of the interesting and curious you may have missed. As usual, science-y stuff first and a rather more mixed bag than normal.
Did you know that for about 2 months of every year there is no night in the UK? No neither did I! This from IanVisits back in May.
Ants that eat electricity are heading for London. No it is 1st April!
[Phobia warning] While we’re on insects, scientists have found a gargantuan aquatic insect in China.
A very rare calico lobster has been caught off the coast of Maine. Rather attractive isn’t it! It’s still alive and on display in an aquarium, but will be returned to the sea later in the year.
On to things that are slightly more concerning. Apparently the environmental cost of beef is ten times that of other meat. But why didn’t they include lamb?
Next an interesting piece on why most of our domesticated animals have floppy ears.
My body makes funny noises. Yours probably does too, but maybe different ones. But why do bodies do these strange things?
Does your rainbow smell? As a “normal” person I find it hard to imagine what synaesthesia must be like. Here are a few insights.
Going back to food for a moment … Scientists are finding a surprisingly complex world of microbes in cheese rind. Yep, that’s what makes all these cheeses taste different.
It looks as if we may have been, and still are being, seriously misled all these years into thinking fat is harmful. Scientists are now suggesting this really isn’t so and dietary advice needs to be changed. Duh!
So stepping quickly into the world of medicine … On how the Great War helped create the 1918 Spanish flu pandemic.
At last some people are beginning to understand the way things work. Here’s a medical study which underlines that decriminalising sex work actually reduces HIV infections as well as violence etc.
Next up we have two interesting articles looking at whether women should or shouldn’t shave areas like legs and armpits: the first by Hadley Freeman in the Guardian; the second by Lucy Brisbane in the Evening Standard. Basically don’t fall into the trap of doing it because fashion etc. say you should. But think about it and shave or not, depending on whether you actually want to, not because of fashion or other people’s attitudes. Be yourself and remember the old adage: “Those that matter don’t mind, and those that mind don’t matter”.
For the historians amongst you, an interesting new theory on how our legends really began.
We’ll gradually bring the historical pieces up to date, so next a look at the naughty and scatological world of medieval marginalia.
A soldier’s lot hasn’t actually changed that much since the Battle of Hastings. Photographer Thom Atkinson displays the essential soldiering kit as it evolved over the last millennium.
Our favourite London cabbie reachee the end of his series on Waterloo Station with a look at the advent of the Eurostar terminal.
This has to be crazy museum piece of the year: an exhibition of broken relationships. Well it is in Brussels.
And finally I’ll leave you with two amusements. First a fractal giraffe. Secondly a display of tooth jewellery.
Anchors away!
Your Interesting Links
More links to items of interest which you may have missed. Quite a science based set this time, although again none of it too deep that non-scientists will get totally lost!
To start off this holiday season, what causes the scent of the sea? And no, it isn’t ozone as everyone believes!

Quickly followed by a quick look at the chemistry of insect repellents.
From insect pests to bacterial pests … A new study suggests that culling badgers is going to have next to no effect on bovine TB and the only way to constrain it is with mass culls of cattle. Sadly there’s probably zero chance the politicians will listen.
Following on from which George Monbiot is (quite rightly) scathing about the way the government is attempting to prevent the reintroduction of wildlife to the UK by using the Infrastructure Bill currently before parliament.
And here’s a piece on how we need to change the way we produce food if we are to be able to feed the ever increasing world population. Basically the whole global food narrative has to change because the current one, even with known tweaks, won’t work!
While we’re on food, here is a piece debunking ten common claims about genetically-modified crops. Yes, I understand the science, but I’m still not entirely comfortable with GMOs.
More food … This time it’s cheese, and a look at the work going on to understand the complex web of bacteria and fungi which turn milk into different types of cheese.
An important article looking at how we have to understand the statistical basis for evaluating actions (medical, social etc.). We have to measure their effectiveness against the background expected death rate (say), rather than against zero deaths.
[Trigger warning, especially for those who may have had miscarriages etc.]
Now let’s slide quietly into the medical arena with a look at the human placenta and the work that is going on to really understand it’s complexity and involvement in gestational and neonatal problems.
Here’s another important piece by the ever-excellent Prof Alice Roberts on how some hormonal contraceptives might be making PMS worse. And apparently this is something many women and lots of GPs do not understand well enough.
Here are twenty things you didn’t know about teeth.
And still on things medical, an interesting article by Carl Zimmer on the mysteries surrounding human blood groups and why we have them.
Now how’s this for a piece of lateral thinking? … A team of scientists are working on a system to use bubble wrap for conducting cheap blood and bacterial tests out in the field, away from the pathology lab, and where cost is a major issue.
The modern bathroom is a wasteful and unhealthy design. But it seems to stay that way because it is space efficient.
So at last we slide into psychology with an article on why the much hated Myers-Briggs test of personality types is totally meaningless.
I don’t pretend to understand Islam, so I found this infographic on the relationship between the various Islamic Sects very illuminating. Now will someone please do the same for Christianity and Buddhism.
And finally … A group of physicists and mathematicians are using mathematical tools to look at the complex social relations in the Icelandic Sagas (as well as other texts) and finding new things that literature specialists haven’t been able to unravel.
NHS Funding
So. According to all the media reports, and the scaremongering from professional bodies, the NHS is in crisis and falling apart because it is significantly under-funded and a political football. It is barely “muddling by” [1,2,3].
Well maybe.
It cannot be denied that the NHS is in crisis. It is badly organised and badly managed. And yes it is a political football.
I’ve written about this before [4,5] and I make no apology for doing so again.
It cannot be denied that some sectors of the NHS are woefully under-funded. This is especially true of GP services where funding has fallen from a high of 11% of NHS budget in 2006 to around 8.3% today against a background of significant increases in the number of consultations and demands from politicians [6].
However overall I cannot believe that the NHS is under-funded. It seems to me the NHS has shed-loads of money to do everything you and I could reasonably want it to do. But that money is badly used, in large part because of the appalling level of wastage.
The NHS employs way more managers and administrators than it needs. That in itself is a huge waste of resources. Just take a look next time you visit a hospital at how many staff are wandering about apparently aimlessly. What do they do? Is it useful? How many are doing nothing but moving pieces of paper from A to B? In this day and age moving pieces of paper around by hand is an inexcusable waste. Do it electronically! Use email, or on-line documents, or database systems.
Yes, to get the NHS using pervasive electronic communication is going to take time, and will need an up-front investment. It will also need the Civil Service and government not to cut corners on cost by being constrained to choose the cheapest bidder, to understand how to manage a big IT project (like don’t keep changing the project scope) and to listen to advice from their trusted suppliers.
The NHS also has far too many managers. Their lives seem to be predicated on bullying staff and chasing meaningless government targets. If we could get rid of the pointless targets and teach the managers how to manage people the NHS would need far fewer of them. In doing this it will take the NHS quite a long way towards trusting and empowering its employees. Trust them to do their job. Trust them with the empowerment to do it efficiently. Empower them to change things sensibly if they can see a better way. In other words, act like a good private company.
Somewhere else the NHS wastes money is in the sheer waste of supplies. One hears stories of hospitals where Ward A needs supply Y but can’t buy it because there’s no money; yet Ward B has a cupboard full of the same supply but has to throw it away because it has gone out of date. In one instance I know of where this happened, and it was pointed out to the top brass by a junior nurse, just changing the procurement policy saved the hospital several million pounds in the first year. Practices like this are not uncommon.
And let’s not talk about hospital food. If patients were fed properly, not only would there be a lot less food waste but the patients might actually get better quicker so they could be discharged sooner.
This is all well and good but I fear it will never happen. For a start politicians, almost by definition, have to keep meddling. Not only is it ideological but it is the only thing they can do to try to show they are doing something.
The other reason it will never happen is that there is no-one at the top of the NHS who has the ability to grasp the whole organisation and energise it. That is not the Civil Service way. But without this there will be no change. The NHS needs someone highly skilled, robust, no-nonsense and bloody-minded to head it up. Someone who will energise the employees, from top to bottom. Who will empower from the top and support empowerment from below. Who will give his or her henchmen a job to do and expect them to get it done — or get out. And most importantly someone who will tell the politicians to butt-out and stay out.
Names like Richard Branson, Alan Sugar and Digby Jones come to mind. You may not like them, but they are the type of people who are needed. Badly needed.
Without someone like this, and without government getting a proper, business-like grip, the NHS is indeed going to go nowhere except, as predicted, down the tubes. And that is something the country cannot afford!
——————————
References:
[1] Observer; 28 June 2014
[2] Daily Telegraph; 18 June 2014
[3] Independent; 29 June 2014
[4] https://zenmischief.com/2014/02/transforming-the-nhs/
[5] https://zenmischief.com/2012/08/reforming-the-nhs/
[6] Royal College of General Practitioners; 27 June 2014
Wearying up to the Weekend
I’m tired. I want to sit and fall asleep but if I do I won’t get any dinner, because the time is approaching.
The week started off quietly, but the last couple of days have been surprisingly heavy.
Yesterday morning Noreen and I had our first introduction to yoga breathing, and some simple yoga. That’s quite tiring because I’m not very flexible (I never was) and not at all fit (entirely self-inflicted). You are also having to concentrate like mad on what you’re being told to do!
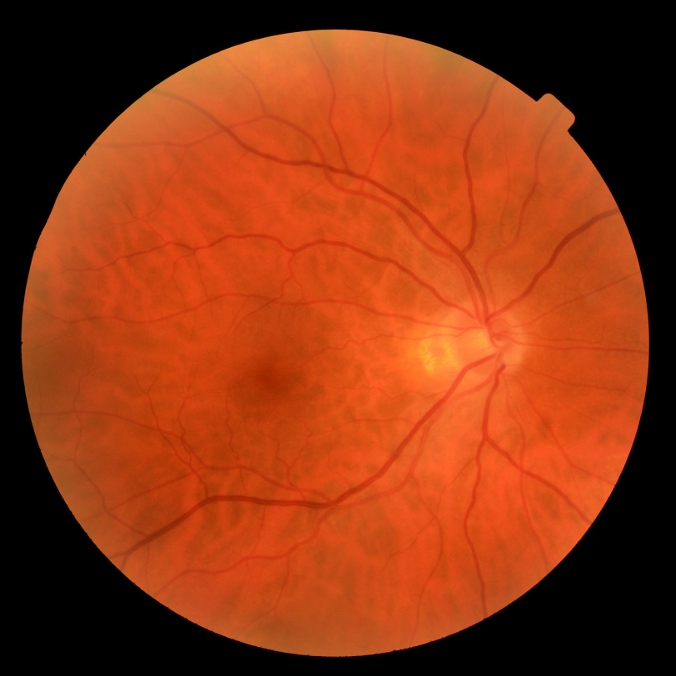
After a quick dash home and some lunch it was off to the optician for my annual eye test. Which is fine, although as I’m diabetic I always get my optician to do a retinopathy scan (basically photograph the back of my eyes). This involves drops in the eyes to dilate the pupils and leaves you unable to focus for several hours. Disorientating to say the least and, as yesterday, it sometimes makes you feel a bit queasy and in need of a lie down. So that too is quite tiring. In fact I often sleep for an hour or so when I get home and my eyes recover.
(Yes, as a diabetic you do get a routine annual NHS retinopathy scan, but I like my optician to do it as well — if only because I get to see the pictures!)
In case anyone is wondering, which is what your retina looks like through a camera lens (this is my right eye yesterday).
Today I have spent the whole day in a training session (on healthcare commissioning, since you ask). On a warm day; in an inside conference room with 15 other people and no control over the aircon. Luckily it was actually interesting, so I didn’t fall asleep despite the temptation!
But brilliant — along the way today I managed to get a couple of things cancelled next week. So I get a free day. Well that’s the current theory, anyway. Better book a day out so we have to get up early!
Arrggghhhh!!!!! But tomorrow it is up early again as it is supermarket day (we normally go on a Friday) and the only sensible time to go is early morning before it gets too busy. Roll up to the supermarket and look to see if there are any good reductions on the meat counter. Then off for coffee and breakfast before tackling the bulk of the job. Hopefully home by mid-morning.
Maybe I get a lay-in on Sunday? Well here’s hoping anyway.
Retirement is such hard work! How do we ever find the time and energy to go to work? Beats me!
Your Interesting Links
More interesting items you may have missed. Lots of science and medicine curiosities in this edition, but its should all be accessible to the non-scientist.
Who thinks mathematics is boring? You won’t when you see the beauty of mathematics in pictures! I’m definitely worried about image four.
Chemicals have a bad name. Wrongly! Manmade or natural, tasty or toxic, they’re all chemicals.
Shifting to the zoo-world, here’s a piece on the curious and improbable tale of flatfish evolution.
Beaver! No not that sort! Honestly your minds! I’m talking about the beavers that have been reintroduced to Scotland, and which are doing well.
Concrete jungle. Yes, it certainly is a jungle out there. Our cities, yes even the most urban and built-up parts of them, can be important wildlife habitat.
Bananas are in trouble and we don’t have a solution to save our favourite fruit. Oh and they’re quite an interesting plant too.
All our food is toxic, innit. Actually, no. But here’s why the fear, uncertainty and doubt are far too easy to believe, and how to counteract it.
On the continuing saga of why chocolate is good for us, but just not in the form you like it.
Five-a-day doesn’t add up. It’s not all marketing hype, except when the arithmetic is wrong.
Turnips. The humble vegetable that terrorised the Romans and helped industrialise Britain.
What do you mean you thought apples grew on trees? Well, OK, they do but originally not the trees you thought. An interesting piece on saving the wild ancestor of modern apples.

Farting well? It could mean you have a good healthy collection of gut microbes.
Just don’t read this next story over dinner. It seems we eat parasites more than we realise.
And another that’s definitely not safe for mealtime reading … A long read on some of the work going on behind faecal transplants, and how they’re being so successful in treating stubborn illnesses.
Lads, here are three cardinal rules from a urologist about care of your plumbing.
Phew! So now let’s leave the scientific and medical behind us and more on.
Naturism is the practice of going without clothes — and it’s not shameful, embarrassing or ridiculous.
Still on naturism, here’s one young lady’s experience of being clothes free at home.
And here are some more views on the way the new Nordic sex laws are making prostitutes feel less, not more, safe.
From
Vagina in the workplace — a story. The closing ideal has to be a good way forward, surely.
Changing tack (yes, OK, about time!) here’s part five of the ongoing series from a black cab driver about Waterloo Station. OK, hands up, how many of you knew it was a war memorial?
And finally, the BBC have unearthed a box of forgotten letters sent from occupied France during WWII. See you never know what’s in that dusty box in the attic!
"Another NHS cock up"
This is an absolutely classic example of why NHS — no actually not just NHS, but all government — IT projects fail so spectacularly.
There are a couple of telling comments in the report on the NHS decision to quietly close the “Choose and Book” outpatient appointments system.
During a recent investigation … MPs were told by NHS staff that while some GPs liked Choose and Book, many did not, and that not all outpatient appointment slots were available on it, limiting its usefulness.
Whether GPs like it or not, that’s the process they have to use; so get on with it and then get it improved. But not having all the appointments there is inexcusable. And the appointments aren’t there; I’ve recently had the run-around getting an audiology appointment because Choose & Book can’t get their act together. (And to be fair my GP went ballistic because of the inefficiency.)
But then it gets worse …
NHS England said … the new e-referral system would use different technology, but it was unable to say how much the scheme would cost.
(Emphasis mine.)
 This is the crux of the matter. If you don’t know how much a project is going to cost, then you do not have a project because you cannot commit funding. There are three prerequisites to running ANY project: a sponsor (ultimate responsibility), a coherent defined and documented set of requirements (the job) and committed funding (ability to pay). Without all three there is no project. Ever.
This is the crux of the matter. If you don’t know how much a project is going to cost, then you do not have a project because you cannot commit funding. There are three prerequisites to running ANY project: a sponsor (ultimate responsibility), a coherent defined and documented set of requirements (the job) and committed funding (ability to pay). Without all three there is no project. Ever.
And government never provide any of the three. They are totally unable to define, specify, cost and manage projects (and they will not take sensible advise from their suppliers). The right level of funding is therefore never committed. And no-one takes overall responsibility.
So things either never happen (because suppliers won’t accept rubbish contracts) or they go tits up (because what is specified either can’t be delivered at the agreed price or isn’t fit for purpose).
So it seems likely that this new project will either be stillborn or will fail within three years. And that is our money — our taxes — down the drain. Again!
Why is there no-one in government, the civil service or parliament with any teeth?
What's that you say?
Now I know I’m getting old. No amend that. I really am well past it!
I’ve been noticing for some time that I’ve not always been hearing everything people say clearly — especially when the person in question is Noreen. So far so normal; we know men never hear anything their wives say! But I was also struggling more and more to hear people talking to me across the table in a noisy restaurant or pub.
A couple of months back, Boots were offering a free, quick hearing test. So I said “yes” and the result was that they said I have noticeable, though not severe, age-related hearing loss. But they would, wouldn’t they! They are in the business of selling expensive hearing aids.
So rather than go their expensive route unnecessarily I went to my GP, who referred me to the local NHS audiology service.
(Our local audiology service is provided by a private company, In Health, as Ealing and Harrow both contract services to “any qualified provider”. They operate out of several local clinics rather than the local hospitals.)
Finally I got to see the audiology people this morning for a much more thorough test — which is all I was expecting to happen. And yes, I do have quite significant drop off in my hearing at middle to high frequencies, which is typical of age-related hearing loss.
Well taht was no real surprise as there is age-related deafness on both sides of my family, as well as my aunt (father’s kid sister) having, I think, had hearing aids since her 40s.
So I have joined the family club with hearing aids!
WHHAAATTTT!!!!
Yes, I have hearing aids!
I really wasn’t expecting that! I was expecting either “you have hearing loss, but it isn’t bad; come for another test in two years” or “yes you need hearing aids, come back in 2 weeks for another appointment and further assessment”. But no, it was “I can do this for you now”.
I’m not sure I really need hearing aids yet, but the advice was that it is better to start with them now, and get used to them, rather than struggle with them later when I really do need them. Exactly the opposite of having glasses.
So I agreed. Because one thing I am determined about is not becoming an awkward old git who denies that they can’t hear, or see, or need help. I remember my parents moaning about their parents being obstinate. And then I watched my parents do exactly the same things my grandparents did! I am determined not to go there. If I do, you have permission to shoot me.
What was amazing about this morning’s appointment was the efficiency of it all — apart from the fact that I was very early and was kept waiting until my appointment time which was tedious but understandable. Then in a 45 minute appointment the young lady tested my hearing quite thoroughly and explained the results. She discussed with me the need for hearing aids. Tried which type fitted me best and she dispensed the hearing aids there and then — setting them up and programming them for me, showing me how they worked, etc.
 I find it incredible that such tiny “in the ear” bud-type hearing aids (that’s them on the right, sitting on a 50p piece) can not only contain their tiny battery, and all the audio equipment, but that they are programmable down a thin wire from a PC.
I find it incredible that such tiny “in the ear” bud-type hearing aids (that’s them on the right, sitting on a 50p piece) can not only contain their tiny battery, and all the audio equipment, but that they are programmable down a thin wire from a PC.
OK the hearing aids are obviously still fairly basic ones, and not adjustable by me, as that’s likely all I need at present. But all this is on the NHS and free of charge. Which I find quite extraordinary. OK yes, that’s maybe how it should be, but I would not have expected at this stage of hearing loss to have qualified for free hearing aids.
When I got home, Noreen was equally incredulous. She has been complaining for a couple of years that I don’t hear what she says to me, but when I told her I had hearing aids, her comment was “Why? You’re not that deaf!”
So there you are … To add to the already old, blind and daft, I’m now deaf as well.
£50m? That Goes Nowhere!
In a widely reported impending announcement David Cameron is allegedly to pledge £50m to fund 1000 GP surgeries (roughly 1 in 8) to open 0800-2000, 7 days a week. See for instance here.
Yes, these extended GP hours are something we, the patients, are asking for. And there is a need because currently there are people (just how many is really debatable) who can’t (for lots of reasons) go a GP appointment but unnecessarily clog up A&E.
But yet again the UK government has proved it doesn’t have a clue about how to actually run the NHS. Cameron doesn’t stand a hope in hell of achieving what he’s pledging, because $50m by my reckoning will pay for a quarter of that for just one year.
Here’s why …
Opening 8-20, 7 days will mean around an extra 34-40 hours a week to be covered. (It’s 34 hours if the practice is currently open 0800-1800, 5 days a week; and many aren’t.)
This means every GP practice which is going to extend their hours, as demanded will need to employ at least one extra full time equivalent GP.
And to cover the extra hours they will also need at least one full time extra member of reception/office staff.
Leaving aside where they are going to find all the suitable, spare GPs, let’s look at the cost. Here’s a very broad brush, back-of-envelope, estimate:
Assume that a GP costs the NHS £150K pa (that’s salary plus pension contributions, plus employers NI contributions, plus other benefits like holiday etc.).
Assume similarly that a full time trained receptionist costs £30K pa (again salary plus benefits package). (Yes you do need trained receptionists; medical work is not something anyone off the street can do, and certainly not safely.)
And then remember that the extra hours will also incur costs for heat, light, hot water and other services — let’s assume that’s £25 per week per practice.
Which means each practice would need funding of around £181K a year.
Dividing that into £50M would provide enough funding for around 275 practices, or about a quarter of what is proposed. And 275 practices is little more than 1 for each NHS area (CCG) in the country (by my count there are 211 of them in England).
So even if the “reorganisation” also provides 100% efficiency savings (which would be a world first!) that still means we’ll achieve only 50% of Cameron’s pledge.
So not only will Joe/Josette Public not realise that this may mean his/her GP isn’t open (and they have to go several miles across the borough to find the practice which is open — on a Sunday when there are no buses), but it is going to go nowhere near meeting Cameron’s pledge.
And that’s without all the fancy gizmos, like Skype video consultations, which are being promised. They have to be paid for too!
Oh and if you read the articles don’t be deceived by all the twaddle about the over 75s. That’s been in the plan for a long time; it isn’t new. Just as I suspect the £50m isn’t new money either.
How do we get these people to understand that healthcare is expensive, that the available funds are being misallocated and mismanaged, and that GP services are hugely underfunded compared with 10 years ago? Because they really don’t have a clue how to fix things.