My latest update on the background to the monkeypox scare.
UK Situation
As of the time of writing the UK has identified 71 cases. [4]
The vast majority of identified cases are isolating at home and do not require hospital admission. [1]
The closest contacts of confirmed cases are being offered the smallpox vaccine. This is the so-called “ring vaccination”. [1]
These closest contacts – anyone who has had direct or household contact with a confirmed case – are being told to isolate for 21 days (ie. the longest incubation period). [1,2]
The same high-risk contacts are advised to avoid immunosuppressed people, pregnant women and children under 12, as these groups are more vulnerable to serious infections. [1]
Contacts are being asked to provide their details for contact tracing. [2]
Sexual Health Clinics are still open for business, but are reported to be doing telephone triage. [4]
Global Situation
More than 131 confirmed cases are being investigated in 15 countries. [4]
More than half the cases are in Spain and Portugal. [1]
The WHO says the outbreak is “containable” and is providing advice to countries on how to tackle the situation. [4]
There seems to be some scaremongering (emanating from the NHS?) that you can be infected by eating meat. [5] Frankly, in my view, this is nonsense. Yes, in theory it may be possible to catch monkeypox from eating undercooked meat from an infected animal – which almost certainly means bushmeat. The chances of a food animal getting monkeypox and getting into the human food chain has to be vanishingly small.
Epidemiology
Genetic analysis of three monkeypox viruses from the outbreak have found it closely matches the virus that spread from Nigeria in 2018 and 2019. [1]
Monkeypox is less transmissible than SARS-CoV-2; the original Wuhan strain had an R0 of about 2.5. Monkeypox has had R0 under 1 in past outbreaks. [3]
A high fraction of SARS-CoV-2 transmission, maybe half(?), comes from people who aren’t showing symptoms at the time; whereas monkeypox transmission before symptom onset seems to be relatively rare, if it happens at all. [3]
The fact that very little if any monkeypox transmission occurs without symptoms means that if people start isolating once they begin to feel sick, they should be able to prevent almost all onward transmission. [3]
Moreover monkeypox spreads slowly (symptom onset is 5-21 days from infection) compared with Covid (symptom onset 1-4 days). [4]
This long incubation time gives contact tracers more time to identify contacts and set up ring vaccination. [3]
Putting that all together suggests that cases are unlikely to rapidly increase and get out of control. [3]
Studies suggest that a Belgian man contracted the virus on a recent trip to Portugal. [1]
The pattern of the outbreak suggests the virus is spreading primarily through sexual networks. [1]
Super-spreader events may have boosted the outbreak since it arrived in Europe. [1] This could be around the rave scene in Spain; a Gay Pride event in the Canary Islands is apparently being investigated. [6]
Cases are being found which have no identified contact with west Africa. [2]
Scientists have a big challenge as they currently do not know how many unreported cases there are; they’re currently seeing only the tip of the iceberg. [2]
Following up on my earlier comment about monkeypox being a DNA virus and different to SARS-Cov-2 (which is an RNA virus), I figured a bit more (very low tech) explanation may help. First off some very simple explanations. (Don’t worry if you don’t know what any of these things are; just think of them as “stuff” or “method”.)
Virus. A pseudo-cell basically composed of some minimal amount of genetic code (DNA or RNA) encapsulated in a lipid (ie. fatty) membrane. It is unable to reproduce on it’s own and has to hijack the machinery of a host cell to make more copies of itself.
DNA. This is the chemical code which holds all our genes. It is composed of the “double helix” of two strands of DNA twined round each other – think of two intertwined springs. In order for the cell machinery to read the text of the DNA the two strands have to be zipped apart and then afterwards zipped back together. Think of this as a whole jumbled box of knitting patterns
RNA. This is essentially a short piece of code created from a piece of a single strand of DNA; it typically provides the instructions for making a single protein. Think of it as a single knitting pattern, extracted from that box of patterns.
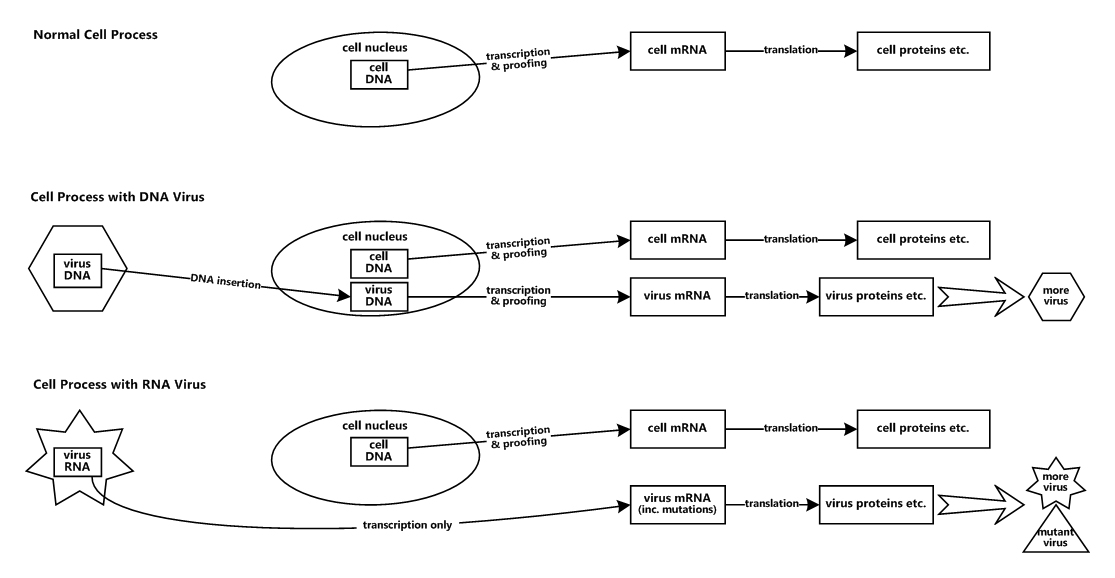
Transcription is the process of unzipping the DNA and copying it to make the RNA; this happens only in the cell nucleus (the strong box which holds the DNA). As in all copying, errors can creep in. So the machinery in the cell nucleus contains a proofreading function which finds the errors and discards the overwhelming majority of them.
There are essentially two types of virus, characterised by how they store their genetic information: DNA viruses and RNA viruses.
DNA viruses (for example, monkeypox) have to insert their genetic code, held as DNA, into the cell nucleus, as that’s the only place where it can be transcribed into RNA. So transcription errors are booted out by the proofreading function and mutation happens very rarely.
RNA viruses (for example, SARS-Cov-2 and flu) don’t have DNA; their genetic code is held as RNA. RNA doesn’t use the cell nucleus for transcription and hence can’t take advantage of the proofreading function. So transcription errors don’t get weeded out and mutations happen very frequently.
The process of using RNA as a blueprint to make proteins etc. is called translation.
And that is an incredibly simplified description of the processes. The details are hideously complex, so hideously complex one can quite see why some people find it hard to believe this has arisen through evolution.
Here’s an equally very simplified diagram (what I drew) of the processes.
Very basic cell process and how it’s used by viruses
Click the image for a larger view
So that hopefully shows why Covid-19 is dangerous, why we need a new flu vaccine every year, and why we hopefully don’t need to be too worried about monkeypox.
Here’s some more background on Monkeypox, following my item from Friday.
Let’s be very clear, right up front … We are not witnessing another Covid, and we’re not days away from lockdowns to contain the spread of monkeypox. However, this is an unusual and unprecedented monkeypox outbreak which has taken scientists who specialise in the disease by surprise – and that’s always a concern. [4]
Spread & Behaviour
Monkeypox is so rare that that most doctors will never see a case in their lifetimes. [2]
Monkeypox is not known to spread easily between people, although cases emerging in several countries at once, and signs of transmission in the community is striking. [1,2]
However the UKHSA saying the risk to the population “remains low”. [1]
The US Centers for Disease Control (CDC) states: “Human-to-human transmission is thought to occur primarily through large respiratory droplets. Respiratory droplets generally cannot travel more than a few feet, so prolonged face-to-face contact is required.” [1]
The virus doesn’t usually spread easily between people as it requires prolonged close contact. [3]
Its R value is generally less than 1, so outbreaks naturally peter out. [3]
Monkeypox can also spread through close contact or by contact with clothing, towels or bedding used by an infected person. [1,3]
It isn’t regarded as a sexually transmitted infection, but it can be passed on during sex via skin-to-skin contact. (This should not be surprising!) [1]
It’s not clear why gay and bisexual men are disproportionately affected. Are sexual behaviours making it easier to spread, or is this just coincidence? After all this is, in general, a community that is more aware of sexual health and getting checked out. [4]
So the latest cases raise many questions and the scientists don’t really have the sense yet of what’s driving this, especially as there’s no travel link that’s identified that links the cases. [2]
So the scientists are very much in response mode: trying to identify cases and trace potential contacts. And because many of the cases don’t join up scientists are aware they’re seeing only the tip of the iceberg. [2,4]
Symptoms
The incubation period between infection and symptoms is long, ranging from five to 21 days. [3]
The first symptoms of monkeypox include fever, headache, muscle aches, backache, swollen lymph nodes, chills and exhaustion. [1]
A rash can also develop, typically on the face first and then on other parts of the body, mainly hands, feet and genitals. The rash can initially look like chickenpox, before forming scabs. [1]
Swollen lymph nodes are a defining feature found in monkeypox but not so common in chickenpox. Currently there are very few kids with monkeypox but the UK is seeing a big surge in chickenpox. So sick kids are more likely to have chickenpox, but be vigilant. [5]
The pictures of large blisters and scabs in the media are an unusual presentation and thought to be more common with the more serious Congo strain of the virus. Most presentation is with small pustules and lesions which are no more than 5mm in size. (Pictures in the references.) [5]
Different Strains
There are two main types of monkeypox: the Congo strain and the West African strain. Only the West African strain has been identified in the UK. [1]
The death rate from the Congo strain is thought to be 1 in 10, whereas it is only 1 in 100 for the West Africa strain.
These are likely to be upper estimates as it is unknown how many (mild) cases go unreported. [1]
It is unknown at this time if the current outbreak is due to a new strain of monkeypox. The sequencing work now being carried out should tell us. [1]
Very early genetic analysis suggests the current cases are very closely related to forms of the virus seen in 2018 and 2019. It is too early to be sure, but for now there is no evidence this is a new mutant variant at play. [4]
Treatments
The antiviral drug tecovirimat is approved in Europe for treating monkeypox, smallpox and cowpox; and approved in the US for smallpox. [1]
The Jynneos vaccine is approved in the US and Europe for preventing monkeypox and smallpox in people aged over 18.
In addition, those who are old enough to have been vaccinated against smallpox as babies should have some protection. Routine smallpox vaccination ended in the UK in 1971 and in the US in 1972. [1]
Pandemic?
Monkeypox isn’t COVID. They’re very different diseases caused by different viruses with markedly different properties. COVID was completely unfamiliar when it first appeared, but monkeypox is a known quantity, and experts on the virus actually exist. [3]
While researchers aren’t completely ruling out a pandemic, they don’t think it is at all likely. [1]
Experts stress that monkeypox is very different from coronavirus. Monkeypox is a DNA virus so it does not mutate as rapidly as Covid or flu. [4]
They’re also saying it’s important not to put this on the same level as a novel coronavirus. [1]
Nevertheless monkeypox is a test of the lessons that the world has (or hasn’t) learned from COVID. [3]
The US, at least, is in a better position with monkeypox than with Covid. They had not planned for a coronavirus pandemic, but they have spent decades thinking about how to handle smallpox bioterrorism. [3]
The UKHSA are saying the risk to the UK population amid the ongoing outbreak “remains low”. [1]
Finally … Be vigilant. If you’re at all concerned phone 111 (in UK) or your doctor. But if you think you might have monkeypox DON’T just turn up at a doctor’s surgery (or sexual health clinic, or hospital); phone ahead so they know you’re coming and can prepare appropriate PPE and protective measures. [5]
OK guys, so here’s another (not quite new) zoonotic disease for us to get our heads round and which piques my forensic nature: Monkeypox.
As of writing there are now 20 cases reported in the UK [1], with over 100 across mainland Europe [5] – where there seems to be a hotspot in Spain – and cases in the US, Canada and Australia. It is being suggested [2] that a number of cases will be being missed due to a similarity with chickenpox.
Monkeypox is a viral disease which is thought to be carried mostly by rodents and is prevalent in remote central and western areas Africa. Cases outside Africa are almost always associated with travel to that continent. That makes the current outbreak in the UK and beyond especially interesting. Although the first reported UK case in early May was in someone recently returned from west Africa, many of the more recent cases apparently do not have an obvious connection to African travel. Perhaps even more interesting is that a significant number of the UK cases are in men who have sex with men (MSM).
The virus is not transmitted in the same way as Covid or flu, but through close bodily contact with an infected person; it can enter the body through broken skin, the airways, eyes, nose or mouth [3]. However it has not previously been described as a sexually transmitted infection – although sex tends to involve close bodily contact! Spread is also possible from infected animals (eg. monkeys, rodents) or from virus-contaminated objects (eg. bedding and clothing).
Unfortunately the initial symptoms are very much like most viral illnesses: fever, headaches, swollen glands, back pain, aching muscles and a general listlessness. Only later does the rash develop; it often begins on the face, and then spreads to other parts of the body, most commonly the palms of the hands and soles of the feet. The rash, which can be extremely itchy, goes through several stages before forming a scab, which later falls off. Although there is no treatment for monkeypox, and no specific vaccine, most cases resolve within 2-3 weeks.
As the name implies, monkeypox is an Orthopoxvirus very closely related to smallpox (also cowpox). The smallpox vaccine is reportedly highly effective protection [3], so anyone who has been vaccinated against smallpox should have some protecton. Have you been vaccinated against smallpox? Smallpox vaccination was compulsory in the UK between 1853 and 1971 [4] so many people over 50 will have been vaccinated, although apparently compliance was falling before the vaccination requirement was removed.
Should we be worried? Current advice is NO. The risk to the public at large is thought to be very low especially as the virus does not spread easily. But then we originally thought that about Covid-19. So no, don’t panic or be alarmed; but do remain alert and if in any doubt about symptoms talk to your GP.
So here’s this month’s selection of links to items you missed the first time and will wish you hadn’t. And of course it’s the usual mixed bag, starting with the hard stuff.
Science, Technology, Natural World
Researchers think they’ve worked out the origin date for the ancient Antikythera mechanism – although they don’t all agree. I find this whole artefact just mind-boggling.
Antikythera Mechanism
A different set of researchers think they’ve uncovered the fossil remains of a dinosaur and some other creatures killed and entombed on the actual day the Yacatan asteroid hit 66m years ago.
Vagina Obscura, a new book by Rachel Gross, reviews the biology of female organs, including the vagina, uterus and ovaries, and how scientists are filling in the gaps in knowledge.
Maybe sometime, maybe soon, medicine will be able to “fix” menstruation.
It seems that peregrine falcons have have made my local (Ealing) hospital their base – well the appalling building has to be good for something!
Giant Orchid (Himantoglossum robertianum)
Meanwhile in Oxfordshire, Giant Orchids (Himantoglossum robertianum) have been found growing wild for the first time in the UK.
It’s being reported that new government rules will provide extra protection for adders and slowworms; which will be good if it happens.
History, Archaeology, Anthropology
A farmer in Gaza has uncovered a 4,500-year-old statue of Canaanite goddess.
Archaeologists at Uruk in Iraq have unearthed, and are trying to recover, an ancient Sumerian riverboat.
Meanwhile in the Assam region of India archaeologists have found more than a few ancient and mysterious giant stone jars.
Still in the ancient world, the grave has been found of an ancient Peruvian who was buried with tools for cranial surgery.
Nearer to home, and to our time, Dr Eleanor Janega, of Going Medieval, looks at the old moneymaking trick of selling indulgences.
Eleanor Janega also writes about a favourite saint: St Sebastian.
In 1580 there was an earthquake, with an epicentre in the Dover Straits, which damaged London’s (Old) St Paul’s Cathedral; needless to say this spawned a flurry of pamphlets – the Facebook of their day.
On another track, IanVisits takes a look behind the scenes at the huge upgrade project nearing completion at London’s Bank Underground station.
Lifestyle, Personal Development, Beliefs
Dungeness (Image: IanVisits)
Oh no! Not again! Yet another item from IanVisits! This time he takes a day trip to Hythe and Dungeness – to explore both and also ride on the Romney, Hythe & Dymchurch Railway.
Shock, Horror, Humour, Wow!
And finally for this month Tom Lamont in the Guardian takes a look at a day in the life of (almost) every vending machine in the world. [LONG READ]
Zoologist Lucy Cooke is waging war on Darwin’s prevailing view of the dominance of males and their benefit from promiscuity. Two articles, the first from the Guardian, the second from New Scientist [£££].
Here’s an interesting article about the work to identify which flu strains to put in this year’s vaccine – and some of the people who spend their lives trying to spot the emerging strains. [LONG READ]
And now another pair of articles, this time looking at the long-term, but haphazard, effect of Epstein-Barr virus, which is responsible for glandular fever. Again the first is from the Guardian, and the second from The Atlantic. [LONG READS]
Environment
One American academic has demonstrated that by just redesigning both homes and industrial processes it is possible to use almost no external power – and overall it is the cheapest solution! And yes, he has actually done it, and lives in the house.
An iconoclastic letter in New Scientist suggesting that as we’ve paved over much of our world we would do well to rip it up and plant trees instead. [£££]
History, Archaeology, Anthropology
1700 years ago a Roman boat sank in shallow waters just off Mallorca on the Spanish coast. Archaeologists are now retrieving the amazingly well preserved cargo.
In what shouldn’t be a surprise the teams restoring Notre Dame in Paris have found early tombs and a lead sarcophagus under the cathedral’s floor.
Despite our misogynistic view, there were female composers in the Renaissance. Now more of the ground-breaking work of Maddalena Casulana has been pieced together and performed.
Now not quite up to date … An expedition has found the surprisingly intact wreck of Ernest Shackleton’s ship Endurance off coast of Antarctica.
Meanwhile a forensic pathologist wishes that a legacy of Covid lockdown is that we change the way we talk about death.
Japan may also need a new narrative as their so-called “killing stone” has split in two, releasing superstition and allegedly a nine-tailed fox. In two stories there’s the usual media-hyped look in the Guardian; however the Japanese think the media have the story wrong as Hiroko Yoda writes on Twitter.
And finally one of the great British train journeys which is high on my bucket list … the longest journey on a single train from Aberdeen to Penzance. I actually want to do Thurso/Wick to Penzance, with Kyle of Lochalsh, Fort William and Mallaig thrown in. I’m not holding my breath in the hope of ever doing it.
Some important prehistoric chalk sculptures, thought to be childhood artefacts, have been uncovered in Yorkshire.
Trousers are one of those wonders of civilisation in that their construction is not overtly simple or logical. So it’s astonishing that the oldest known “pants” seem to have originated in Asia, and a pair is survived around 3000 years. And the weaving is absolutely amazing.
Earlier this week there was a long read article in the Guardian by Dr Clare Gerada, a senior GP and former chair of the Royal College of General Practitioners. In the article Dr Gerada draws on her own experience to show how the GP’s role has changed in the last 30 years. No wonder the NHS is haemorrhaging GPs because it is not a pretty tale.
So our pathetic government appear to have decided that all Covid-19 restrictions will be removed in two weeks time, as part of the plan to save Boris’s skin. Basically they seem to be saying that Covid is over, the case numbers are falling rapidly, there’s no longer any need to isolate, and we can all go back to normal. [1,2] Essentially this says “we don’t care; go back to normal; if you get Covid well tough luck, but it is now only a cold so continue going to work and spreading the disease further”.
Let’s look at this.
Of course the government reported case numbers are falling; they’re designed to. People are being urged to go back to work, and testing is not being pushed. There is now no requirement to get a confirmatory PCR test following a positive LFT; and there’s no requirement to log the result of a LFT; so testing has dropped off a cliff – people just aren’t bothering. So as the government reports only confirmed positive tests, of course their numbers are falling.
However this does not accord with data from the Office of National Statistics (ONS; a government body) who do random sampling of the population. Nor does it agree with the data from the Zoe Covid Study, who track reports from their 4 million subscribers. [3,4,5] The Zoe study is showing rates still incredibly high at around 200K/day (as it was at the beginning of January) and the ONS data is tracking this fairly closely. That means around 1 in 25 people currently have Covid [5] and anything up to 10% of those are re-infections [3,5].
But it is worse than this …
Going back to normal, means no testing and no isolation. So people will be walking around with Covid as they think they have a bad cold (or are even asymptomatic), they’ll keep travelling and going to work/school, and spreading infection. Many will be forced back to work as many employers won’t tolerate time off sick with a cold (which is in itself stupid, but part of the “work at all costs” ethic).
More people walking about spreading infection means that the number of cases will rise, as will hospitalisations and deaths. And because there’s no testing the government won’t know, until hospitalisations, deaths or school absences start climbing out of control. But by then it is too late; the genie is out of the bottle. (Remember that hospitalisations and deaths lag behind infection by 2, 4 or even more weeks.)
That in turn puts the vulnerable at even greater risk. And many vulnerable people (like me) are feeling even more that they’re condemned to “house arrest” because they dare not risk going out and getting infected.
It also means more children off school, or having their education impacted because their teachers are sick.
And the higher the rate of infection, the higher the number of cases of Long Covid which will severely impact the patient’s life for … well we don’t know how long!
More infection also means the virus has even greater opportunities to mutate. That’s the way evolution works. These new variants may be less or more infectious, and/or cause more or less severe infection. And again we wouldn’t know, because there’s no testing.
All this is compounded in that immunity wanes. We know that the good immunity provided following two vaccinations was falling off rapidly after 6 months [7]; hence the booster programme. But it does now seem that immunity provided by boosters falls off rapidly too, such that someone like me who had their booster in mid-October (17 weeks ago) now has almost no benefit from it [6]; I’m back where I was last June with a risk of around 4 times the norm [8] (and I’m by no means in the extra-super-mega-vulnerable range). We seem to be needing a new booster every 3 months or so, but there appears to be no plan for this – indeed the current booster programme has effectively stalled [3].
According to the BBC “The law will be replaced with guidance … and for example people will be urged not to go to work if they have Covid” [2]. Frankly the government can provide as much guidance, urging and recommendation as it likes, but people are going to take little notice: they need to work and their employers aren’t going to tolerate high levels of absence.
Is it any wonder the vulnerable and the disabled are worried. They feel that the government doesn’t care about them and wants them out of sight and out of (their) mind. (From a personal perspective, friends are going to increasingly not understand of one’s avoidance of social gatherings etc.)
I have seen a number of respected scientists, including some members of Independent SAGE [9], suggesting that the government’s proposed action is nothing less than “criminal negligence”. We don’t know what is round the corner in terms of new variants, so they could well come back and bite us in the bum at any time. And when it does the consequences are going to be a direct result of yet further government failure.
Whether it is actually “criminally negligent” only a court could decide, but I would certainly class it as totally stupid and intensely unethical.
















 Earlier this week there was a long read article in the Guardian by Dr Clare Gerada, a senior GP and former chair of the Royal College of General Practitioners. In the article Dr Gerada draws on her own experience to show how the GP’s role has changed in the last 30 years. No wonder the NHS is haemorrhaging GPs because it is not a pretty tale.
Earlier this week there was a long read article in the Guardian by Dr Clare Gerada, a senior GP and former chair of the Royal College of General Practitioners. In the article Dr Gerada draws on her own experience to show how the GP’s role has changed in the last 30 years. No wonder the NHS is haemorrhaging GPs because it is not a pretty tale.